Lumbar Microdiscectomy
Prime Suspect: Herniated Disc
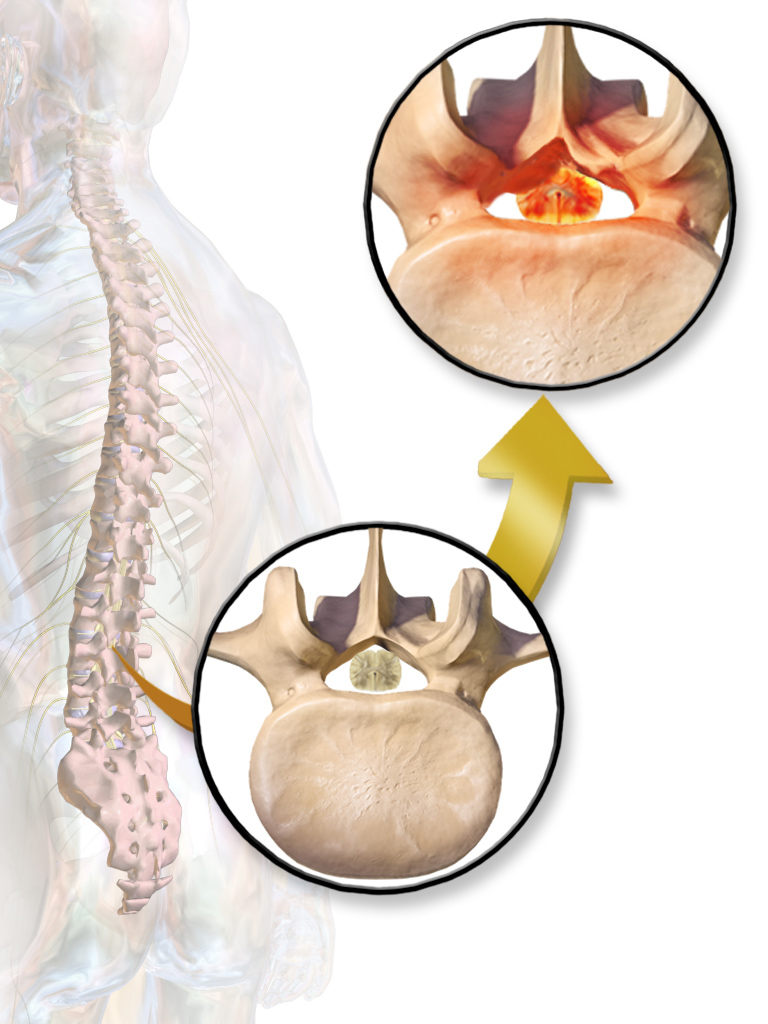
A herniated disc is a common injury that can affect any part of the spine. A herniated disc can cause severe pain and other problems in the arms or legs.
Discectomy is surgery to remove lumbar (low back) herniated disc material that is pressing on a nerve root or the spinal cord . It tends to be done as microdiscectomy, which uses magnification to view the disc and nerves.
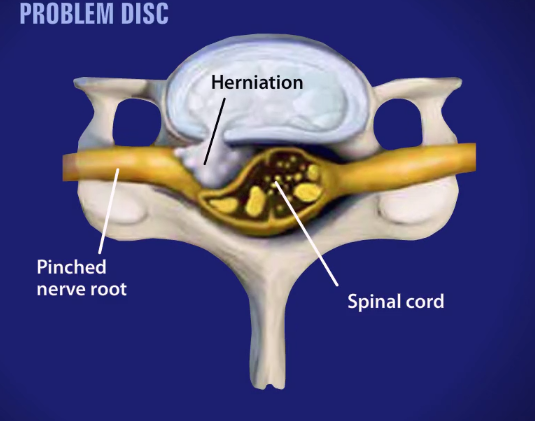
Above you can see the blue herniated disc protruding out of its normal space and pressing into the nerve. The red indicates that the nerve is now sending painful signals that will be stopped once the surgery is done successfully.
Surgery Overview: Lumbar Microdiscectomy
A lumbar microdiscectomy surgery is performed to remove the portion of a herniated disc that is irritating or inflaming the nerve root.
We begin the surgery through a small incision in the midline of the low back.
First, the back muscles, called erector spinae, are lifted off the bony arch, called the lamina, of the spine. Since these back muscles run vertically, they can be moved out of the way rather than cut.
The surgeon is then able to enter the spine by removing a membrane over the nerve roots.
Often, a small portion of the inside facet joint is removed both to facilitate access to the nerve root and to relieve pressure over the nerve.
The nerve root is then gently moved to the side and the disc material is removed from under the nerve root. Only the herniated portion of the disc is removed; the healthy portion of the disc is left intact.
Recovery
A Lumbar microdiscectomy has become the gold standard for surgical intervention for lumbar disc herniation. The procedure was first reported in 1976. With more than 40 years of experience in the hands of many practitioners, lumbar microdiscectomy has stood the test of time.
I began to do lumbar microdiscectomy as an outpatient procedure in 1990 and published my results in what was then the largest reported series of outpatient microdiscectomies in 1994. The procedure has high success rates and low complication rates. Generally speaking, early recovery and return to function, especially sedentary or light duty positions, are common.
Patients can generally drive within a week to 10 days and return to sedentary types of positions within 2 to 4 weeks.
![]()